.png)
.png)

Can Psychiatrists Help With Sleep Issues? The Anxiety-Insomnia Trap
Most of us have nights where sleep dodges us, but when anxiety tags along, it turns into a vicious cycle. Anxiety cranks up your brain's alarm system, flooding you with racing thoughts that block rest. Poor sleep then amps the anxiety, making everything feel heavier. Studies show that insomnia acts as a risk factor, with chronic cases raising the odds of developing anxiety disorders—sometimes doubling the vulnerability over time.
In clinics, this overlap hits hard: 25-45% of folks with anxiety disorders battle severe insomnia symptoms, while about 10% of adults experience chronic insomnia and 30% report brief symptoms. Psychiatrists step in here, using tools like DSM-5 assessments to spot if it's standalone insomnia or tied to anxiety. They check medical culprits too, like thyroid issues, ensuring nothing's overlooked. The good news? Addressing it early breaks the loop, leading to clearer days and deeper nights.
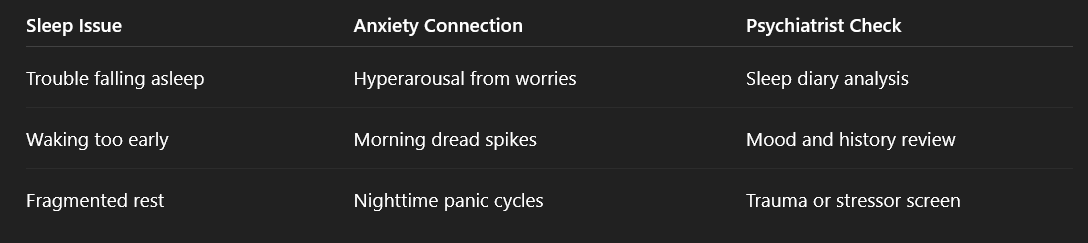
Here's a simple breakdown of how these issues connect:
How Psychiatrists Tackle Sleep Issues: Core Treatments
Psychiatrists don't just hand out pills—they craft plans that fit your life, starting with the gold standard: Cognitive Behavioral Therapy for Insomnia (CBT-I). This isn't fluffy advice; it's a structured 6-8 week program with proven punch, boosting sleep efficiency by 8-16% and adding 30-60 minutes of real rest per night. Components like sleep restriction (curtailing time in bed to build drive) and stimulus control (bed for sleep only) rewire habits gently but effectively.
For anxiety-fueled insomnia, they often sequence it smartly: Tackle anxiety first with CBT or meds like SSRIs, then layer in CBT-I. Research backs this—treating anxiety upfront yields meaningful sleep gains, with sequential approaches boosting response rates to 50-68% in comorbid cases. Meds play a supporting role: Dual orexin receptor antagonists (DORAs) like daridorexant quiet wake signals without next-day grogginess, delivering solid results even in mood disorder patients.
Key approaches psychiatrists use:
- CBT-I first-line: 70-80% efficacy long-term, with low relapse risk.
- Sequential therapy: Anxiety treatment then insomnia focus—superior response (50-68%) for combined issues.
- Targeted meds: SSRIs for root anxiety (improve sleep quality and add ~42 minutes duration indirectly); DORAs for pure insomnia (40-50% response). Short-term use prioritized.
- Combo power: Behavioral first, then meds if needed—response jumps from ~40-50% to 60-68%.
This personalized path feels empowering, not overwhelming, because it meets you where you are.
Evidence That Psychiatrists Help With Sleep Issues
The data speaks clearly—psychiatrists' strategies deliver because they're built on decades of trials. CBT-I outperforms meds alone for lasting change: While drugs' effects fade post-treatment, CBT-I holds gains up to 24 months, with about 45% of patients achieving significant increases in nightly sleep time (average +30-50 minutes). In anxiety-insomnia combos, untreated sleep problems raise depression risk 2-5 times down the line, but targeted care reverses that trajectory.
Recent studies shed light: Daridorexant reduces insomnia symptoms in patients with bipolar and unipolar mood disorders, with sleep improvements tied to better mood regulation.
Sequential therapy delivers too—prioritizing anxiety treatment first accelerates remission, boosting overall response rates to 50-68% in comorbid cases. In primary care, 20-50% of patients report insomnia symptoms, yet it's often under-discussed (only ~25-50% raise it)—psychiatrists close that loop effectively.
Compare top options side-by-side:
.png)
These results—from AASM guidelines and major RCTs—make relief not just possible, but predictable.
When to Seek a Psychiatrist for Sleep Issues
Not every rough night calls for a specialist, but certain signs signal it's time to reach out. Chronic insomnia—lasting three months or more—disrupts life deeply, often signaling deeper anxiety ties that self-help can't fully untangle. Daytime exhaustion fogging your focus, straining relationships, or tanking productivity? That's a clear red flag.
If anxiety meds leave sleep untouched, or tools like the Insomnia Severity Index (ISI) score you moderate-to-severe (14+), psychiatrists offer the full diagnostic edge—meds, therapy oversight, unlike psychologists, limited to talk.
Start simple to build momentum:
- Track one week's sleep patterns: Note fall-asleep time, night wakings, and morning grogginess on a scale of 1-10.
- Jot symptoms and triggers: Racing thoughts? Caffeine habits? Past fixes like melatonin that flopped?
- Book that first consult: 30-45 minutes via India's telepsychiatry (Practo, Rocket Health)—no GP referral needed, just honest prep.
Psychiatrists shine for mental health-sleep links; sleep specialists handle apnea via studies. Acting early stops the anxiety-insomnia spiral from worsening.
Practical Steps and Hope Ahead
While waiting, layer in basics that amplify pro care. Dim lights an hour pre-bed to cue melatonin; skip caffeine after noon to quiet your system. These aren't cures but bridges to deeper fixes like CBT-I, where experts refine them.
Post-consult expect:
- Sleep logs for patterns.
- Digital CBT-I apps for home practice.
- Follow-ups (2-4 weeks), tweaking meds or therapy.
Relief unfolds gradually—many notice lighter nights in weeks, steady rhythm in months. You're not flawed; these are common, solvable challenges. Track this week, connect with a psychiatrist from Rocket Health—rest awaits. You've got this.

.jpg)
.jpg)
.jpg)